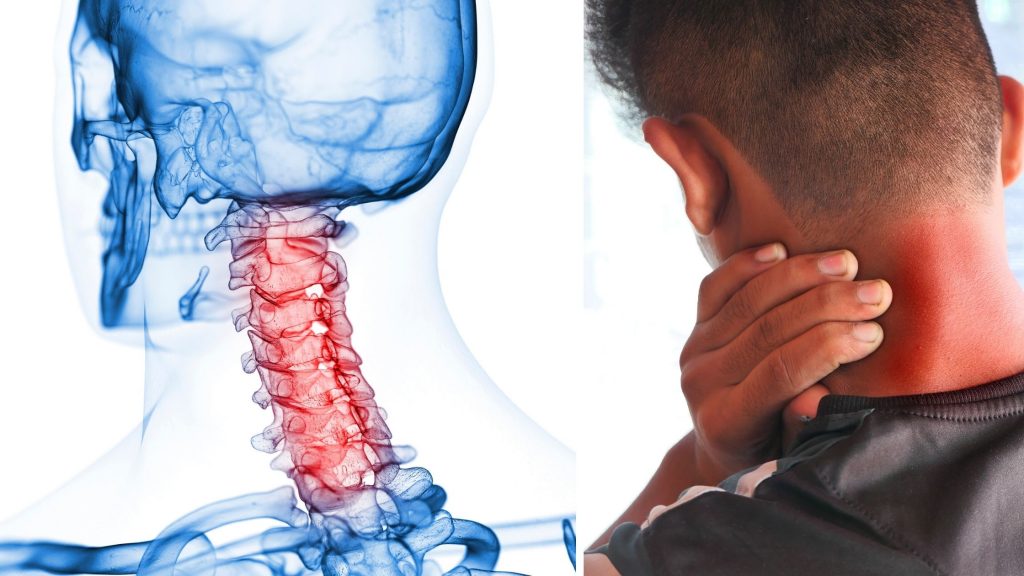
Effectively managing upper limb spasticity is one of the biggest challenges after a stroke. This complication, often presenting in a flexor pattern, can severely limit a patient’s recovery and functional independence.
In this comprehensive guide, you’ll learn a proven 3-step method to assess and treat post-stroke spasticity using evidence-based Neurodevelopmental Treatment (NDT) principles.
Step 1: Observation- How to Recognise Spasticity in Stroke Patients
The first step of assessing the spasticity in a stroke patient is observation. We have to observe for elbow flexion. In stroke, the spasticity can develop either in a flexor pattern or in an extensor pattern.
Since the flexor pattern is more common3, we will discuss the assessment and treatment of flexor spasticity.
We will discuss the assessment process in reference to the demonstration “Comprehensive management of stroke” that we had on the 7th of September, 2025, by Dr B.K. Nanda (Senior Lecturer, SVNIRTAR) on the occasion of World Physiotherapy Day. The screengrab is from the demonstration.
Ask the patient to raise the arm. When observing a stroke patient raising their arm, you’ll notice the elbow remains flexed. Observe the two cases in the image below.
The female stroke sufferer has significant flexion spasticity as compared to the male. This common presentation results from spasticity in the elbow flexor muscles. By observing the raised arm, we can also predict the Brunnstrom staging of the stroke recovery. It is important for planning the rehabilitation progression.

The symptoms of flexor synergy in the upper limb after stroke are:
- Scapula retraction and elevation,
- Shoulder abduction and external rotation,
- Elbow flexion,
- Forearm supination,
- Wrist and finger flexion.
Both patients (in the image) have different grades of spasticity. We will progress this article with the male patient in the image. But before that, we must also learn which component is causing this spasticity.
What Are the Neural and Non-Neural Causes of Spasticity?
Spasticity has two different components. It is important to find out the component of spasticity as treatment depends on it2.
Neural Component:
- Caused by hyperactive stretch reflexes
- Develops in the acute phase following stroke
- Associated with abnormal synergy patterns and hypotonia
- Responds to neurophysiological treatment techniques
Non-Neural Component:
- Results from adaptive positioning and secondary changes
- Develops over time due to prolonged flexed positioning
- Includes joint capsule tightness, skin contractures, and muscle fibre shortening
- Requires mechanical stretching and positioning interventions
Step 2: Examination- Step-by-Step Spasticity Examination for Stroke Rehabilitation
After observation comes the examination, where we will quantify the grade of spasticity. We will use various manual techniques for examination.
However, in a recent advancement, a markerless motion capture system is used to quantify abnormal flexor synergy. It can quantify it in seconds, offering clinicians precise, objective measurements to complement traditional assessment methods3.
So, here is the exact process of manual examination of the upper limb for spasticity in a stroke patient.
Patient Positioning:
Always examine spasticity with the patient lying down, not sitting. Anti-gravity postures increase spasticity, making assessment less accurate. The patient should be comfortable and relaxed in the bed.
Why Movement Speed Matters in Spasticity Testing:
Use high-velocity, quick movements to test spasticity. This is important because low-velocity or sustained stretching is used for the treatment of spasticity rather than assessing it.
Quick stretches stimulate the muscle spindle and activate the stretch reflex, revealing the true degree of spasticity.
Modified Ashworth Scale: How Is Spasticity Measured?
When performing the quick stretch test, you’re looking for the characteristic “catch” that defines the grade of spasticity. Observe the image below. The sudden jerk at the beginning of the movement is the catch.

This is the grade 1 spasticity based on MAS. This is because in grade 1 spasticity, you will get CATCH either at the beginning or at the end of the sudden movement.
Think of it like eating rasagulla, that delicious Indian sweet. We typically eat rasagulla either at the beginning of our meal or at the end – normally at the end.
Sometimes we prefer to have rasagulla at the beginning, then go for the main course, and at the end we don’t take rasagulla because we’ve already had it. Those who ate rasagulla at the beginning won’t take it at the end.
Similarly, if we get a catch at the beginning of the movement, we won’t get a catch at the end range. If there’s no catch at the end range, then we’ll get it at the beginning.
This simple analogy helps remember that the spastic catch occurs at one point in the range, not throughout the entire movement.
Grade 1 Spasticity:
Increased muscle tone with a catch followed by release, or minimal resistance at either the beginning or end of the range of motion.
Why Does Slow Stretching Help Spasticity?

Now, observe the slow movement on the same hand of the same patient. There is no catch. So, why does a slow, sustained stretch not produce catch?
This is due to a mechanism known as autogenic inhibition.
What Is the Autogenic Inhibition Reflex?:
Autogenic inhibition reflex is a sudden relaxation of a muscle upon the development of high tension. It is a self-induced, inhibitory 1.
Here’s how it works mechanically:
- Slow stretching stimulates the Golgi tendon organ (GTO) present on the tendon
- Type 1B afferents carry signals to the posterior horn cell
- The stimulus travels from the posterior horn cell through connecting neurons to the anterior horn cell of the same muscle (for example, from C6 to C5)
- This inhibits the alpha motor neuron, reducing muscle tone and causing the muscle to fail to contract.
- The same muscle that’s being stretched ends up inhibiting itself through this reflex mechanism
Think of this concept like a personal example: If you fail an exam, you become inhibited – you might cry because you failed the examination, and you’re emotionally inhibited. Similarly, the same muscle’s afferent nerve fibres will inhibit the same muscle’s alpha motor neuron.
How Slow Stretching Improves Muscle and Joint Health:
Slow stretching also addresses non-neural components by lengthening shortened tissues, including skin, joint capsules, and muscle fibres.
Step 3: Choosing Right Spasticity Treatment Based on Assessment
Observation guides examination priorities. Now, observe the screengrab from the presentation again. We notice elbow flexion during arm elevation but normal extension when the patient is relaxed and lying down.
This suggests that the spasticity in the patient is primarily due to a neural component rather than a non-neural one. Non-neural contractures would maintain the flexed position regardless of the patient’s posture or activity level.
NDT Techniques for Treating Spasticity in Stroke Patients
Since the spasticity is primarily due to the neural component, our treatment will be based on the NDT approach.
The Neurodevelopmental Treatment technique, developed by Dr. Karel Bobath (neuropsychiatrist) and Mrs. Berta Bobath (physiotherapist), uses reflex inhibitory patterns with key point stimulation.

Key Points:
- Scapula (primary proximal key point)
- Arm (secondary proximal key point)
How to Apply NDT Scapular Protraction for Elbow Extension:
Position the patient leaning forward with hands clasped. This scapular protraction naturally promotes elbow extension through the reflex inhibitory pattern. Place one hand over the scapula and the other on the lower arm, facilitating the movement without restricting the elbow.
Functional Activities to Improve Spasticity Outcomes
Transform therapeutic exercises into enjoyable activities. Instead of simply asking patients to lean forward, place a basketball or a volleyball on a stool in front of them. Have them lean forward to grasp the ball, lift it, and throw it back to you. This approach:
- Motivates patient participation
- Combines scapular protraction with elbow, wrist, and finger extension
- Provides functional movement patterns
- Makes therapy feel like play rather than work
You can even make it more interactive by having them reach forward to pat your upper back – patients enjoy this type of functional, engaging movement much more than abstract therapeutic commands.
What Results Can Be Expected from NDT Treatment?
For patients with Grade 1 spasticity, as demonstrated, consistent application of these techniques typically shows good results. Those with Grade 2 or Grade 1+ spasticity will show more dramatic improvements with the reflex inhibitory pattern technique.
Remember, proper assessment guides appropriate treatment selection. When neural components dominate, focus on neurophysiological techniques like NDT.
When non-neural components develop, incorporate mechanical stretching and positioning strategies alongside the neurological approaches. After consistent treatment, you’ll find the elbow stays straighter during functional movements, and there’s typically no need for orthotic devices.
Keep Reading: 7 Easy Exercise for Paralyzed legs at Home to Improve Walking
FAQ
The author is a physiotherapist who has been practising for the last 17 years. He holds a Bachelor's in Physiotherapy (BPT) from SVNIRTAR (Swami Vivekananda National Institute of Rehabilitation and Research), one of the prestigious physiotherapy schools in India.
Whatever he learns dealing with his patient, he shares it with the world through blogs and e-books. He also owns a YouTube channel, "Sunit Physiotherapist" with over 8 lakh active subscribers. Here, he shares everything he gets to learn serving the patient.